Altered Mental State
Altered Mental State (AMS) refers to any change from a person’s normal level of consciousness, awareness, thinking, or behavior. It is a broad clinical term used to describe abnormalities in alertness, cognition, orientation, perception, or responsiveness.
🧠 Key Characteristics of AMS May Include:
- Confusion – inability to think clearly or concentrate
- Disorientation – not knowing time, place, or identity
- Lethargy – drowsiness or decreased alertness
- Delirium – sudden onset confusion, often fluctuating
- Stupor – unresponsiveness, but can be aroused with strong stimuli
- Coma – complete unresponsiveness
- Hallucinations or delusions
- Agitation or inappropriate behavior
The primary focus of the ED evaluation of a patient with altered mental state (AMS) is as
follows:
- To address easily reversible causes, e.g. hypoxaemia, hypercarbia, and hypogłycaemia.
- To differentiate structural from toxic-metabolic causes since the former require emergent central nervous system imaging, whereas the latter are usually more readily identified by laboratory studies.
SPECIAL TIP FOR GPs
– Always consider reversible causes of AMS that you can initiate treatment for in your office:
e.g. hypoglycaemia (oral sugar or IV Dextrose 50%), hypoxaemia (supplemental oxygen), or
heat stroke (cooling measures and IV normal saline), before sending the patient to the ED
by ambulance.
Management
Initial priorities
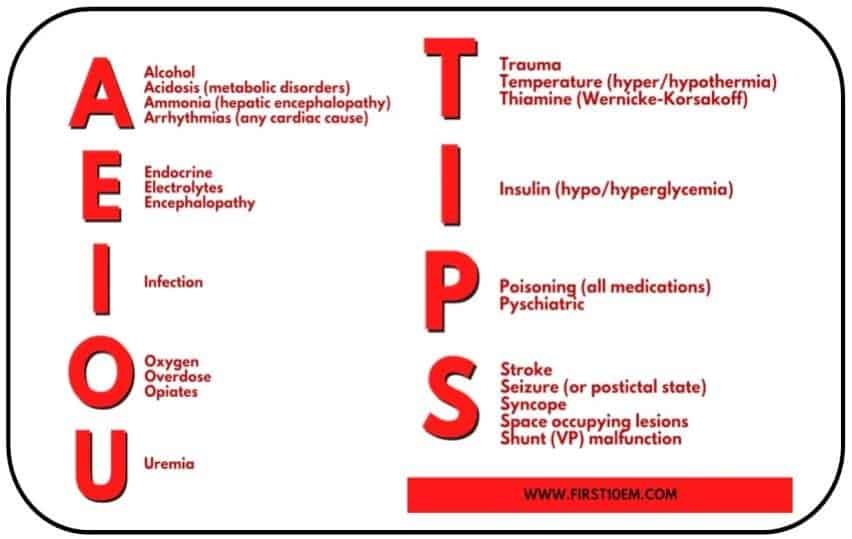
- See Figure 1 for approach to differential diagnosis of altered mental state.
- The patient should be managed initially in the critical care area.
- If a promptly reversible cause of AMS is found, then the patient can be downgraded to the
intermediate acuity area.
Positive airway control/C-spine immobilization.
- Open the airway and search for foreign bodies.
- Insert oral or nasopharyngeal airway.
- Apply stiff collar or manual immobilization if history does not exclude trauma.
- Definitive airway if patient is comatose: intubation with/without rapid sequence intubation or perform surgical airway such as emergency cricothyrotomy.
Oxygenation/ventilation.
- Provide supplemental high-flow oxygen.
- Institute hyperventilation in moderation to achieve a PCO, between 30-35 mmHg if
there are indications of raised intracranial pressure. In general, the PCO, level should be
between 35-40 mmHg.
FIGURE 1 : Approach to differential diagnosis of altered mental state

Cardiac output.
- Check that there is a major pulse; if not, start CPR!
- Obvious external haemorrhage should be stopped with direct pressure only.
Do stat capillary blood sugar.
Monitoring: ECG, pulse oximetry, vital signs q5-15 minutes.
Start peripheral IV at a slow rate (unless hypoperfusion present) with isotonic crystalloid.
Labs : FBC, RP, electrolytes, ABG (look for metabolic acidosis and hypercarbia).
NOTE
CO2 narcosis does not necessarily present with respiratory distress; they are usually in respiratory depression. Consider serum calcium, drug screen, serum ethanol, carboxyhaemoglobin level, and GXM.
AMS cocktail: consider its use in part or whole.
- D50% 40 ml IV if patient is hypoglycaemic, followed by infusion of D10% over
3-4 hours. - Naloxone (Narcan®) 0.8-2.0 mg IV bolus.
- Thiamine 100 mg IV bolus in alcoholics or malnourished patients.
- Flumazenil (Anexate®) 0.5 mg IV bolus.
- Can be repeated within 5 minutes if necessary.
- Do not use empirically unless the history is strongly against a mixed OD. If the patient has been taking cyclic antidepressants or is taking chronic benzodiazepines for fits, unnecessary use of Flumazenil may produce intractable fits.
- X-ray cross-table lateral film of C-spine if trauma cannot be excluded.
TABLE 1 Clues from history and physical examination pointing to causes of AMS
| Non-structural cause | Structural cause |
|---|---|
| Empty pill containers | Complained of headache to family/friends prior to AMS |
| Medical diseases, e.g. epilepsy, liver disease, diabetes, etc | History of brain tumour |
| Possible CO exposure | Trauma |
| Absence of focal neurological signs | Presence of focal neurological signs |
| Signs of metabolic acidosis | |
| Anticholinergic signs |
Clinical evaluation: the focus is on differentiating structural from toxic-metabolic causes of
AMS (Table 1).
History: rarely clear-cut; look for clues from patient’s family, friends, belongings, and
information scene from paramedic/ambulance officer.
Examination: brief external assessment of patient searching for stigmata of numerous disease processes. While a head-to-toe examination is important, in AMS pay most attention to a focused neurological examination.
AMS due to suspected structural causes
1. Give supplemental oxygen to maintain SpO, of at least 95%.
2. Start IV at a slow rate.
3. Perform head CT scan.
4. Lower intracranial pressure if indicated.
- Controlled ventilation: works fastest.
- IV mannitol is useful in conjunction with neurosurgical consult. Dose is 1 g/kg body weight (BW), i.e. BW x 5 mls/kg BW of 20% mannitol solution.
- Steroids are debatable.
AMS due to suspected toxic-metabolic causes
1. Do gastric lavage; to be performed with airway protection if required.
2. Use activated charcoal in suspected drug overdoses.
3. Check rectal temperature and consider heat stroke if temp >40°C and taking anticholinergics.
4. If meningitis is suspected, consider early lumbar puncture (after CT head scan). Start empiric antibiotics before either of the tests together with a neurological consult.
Dispositioп
Admit all cases of AMS. Admit to ICU those who are intubated or exhibiting haemodynamic instability.
Reference : Guide to the Essentials in Emergency Medicine 2nd Edition, Shirley Ooi